2.1 Survivor journeys
Survivors’ journeys are diverse, ranging from those with minimal impairments to those requiring lifelong care. Many return home but struggle with hidden disabilities. Lived experiences reveal common themes: initial relief gives way to frustration with unmet needs.
Case study: MacLean MacLeod (Forres, Moray)
Cardiac arrest
MacLean MacLeod, a fit member of the Findhorn Coastal Rowing Club, experienced an OHCA on 21 April 2022, after a high-intensity training row. Thanks to the swift actions of his teammates, who recognised the arrest immediately, performed CPR, and used a nearby defibrillator, MacLean’s life was saved. MacLean spent nearly three weeks in hospital, where he received excellent acute care, including the fitting of three stents.
Problem after cardiac arrest
Once discharged home, MacLean and his wife found it difficult to navigate recovery without clear guidance or follow-up. Despite repeated attempts to secure appointments, there was no structured pathway. “I felt abandoned, like I was left to figure out recovery alone,” he recalled.
Progress only came after contacting his local MSPs in early 2023. MacLean’s experience highlights how even when emergency and hospital care are exemplary, the absence of a clear, coordinated pathway after discharge can leave survivors and families feeling isolated and unsupported. Support from Keiran’s Legacy, RCUK, and Sudden Cardiac Arrest UK (SCAUK) provided vital peer connection and information, emphasising the importance of embedding recovery and aftercare within a national quality standard.
Case study: Ruth Harvey (Taunton, Somerset)
Cardiac arrest
Ruth Harvey, 55, experienced an OHCA on 11 July 2021, while walking in Salisbury. Thanks to her partner providing CPR and a rapid ambulance response, she survived. After around 25 minutes, paramedics detected a faint pulse, though Ruth remained unconscious for several days.
Problem after cardiac arrest
Following three days in intensive care, Ruth awoke with memory loss and delirium. Ruth was discharged after three weeks with no cardiac issues identified, but she faced severe fatigue, neurological symptoms, and PTSD “I was lost, struggling to remember simple things, and the fear of it happening again was crippling,” she said.
Ruth learned pacing strategies, such as breaking tasks into 15-minute intervals, through self-referred neurology support. Her partner, Simon, faced ongoing anxiety from performing CPR, with no professional support. SCAUK and Headway ultimately provided vital support for both Ruth and her partner, but their intervention also highlights the absence of coordinated clinical care for cardiac arrest survivors and key supporters.
Case study: Alan Owen (Llanddarog, Carmarthen)
Cardiac arrest
Alan Owen, an IT consultant, experienced an OHCA on 3 April 2022, during a walking football match. Revived after CPR and three shocks from a defibrillator, he was diagnosed with hypertrophic cardiomyopathy and fitted with an implantable cardioverter defibrillator (ICD). His son, who witnessed the event, developed anxiety. “Every day I worried about the ICD shocking me again, it was a shadow over my life,” Alan shared.
Problem after cardiac arrest
Despite excellent in-hospital care, he lacked mental health support, still awaiting an appointment one year after referral in 2023.
Peer support from Cardiomyopathy UK and Wales Air Ambulance’s aftercare service helped him reframe fears and return to work. Alan’s experience emphasises the need for ongoing psychological support for survivors and key supporters, highlighting gaps in care pathways that the QS could address.
Case Study: Siobhan Wren (Wisconsin, US/Manchester, UK) (Key supporter: Josephine Wren)
Cardiac arrest
Siobhan Wren, a healthy 20-year-old studying abroad in the US, experienced an OHCA while shopping with friends in Wisconsin. CPR was started by a police officer without access to a defibrillator, and after resuscitation, she was placed in a coma. Her parents travelled from the UK and were faced with limited communication and little emotional support.
Problem after cardiac arrest
Although Siobhan survived and received an implantable cardioverter defibrillator (ICD), the family left hospital with minimal understanding of her condition, and on returning home, she experienced further shocks, unclear follow-up, and no guidance on lifestyle, risk, or psychological impact. A later collapse in Manchester led to a month-long admission, during which her mother and key supporter, Josephine Wren, again struggled to navigate support as the parent of a young adult.
Positive interactions — including follow-up contact from the police officer and first responders, clear written explanations to help Siobhan understand her condition, a supportive consultant, and peer networks such as SCAUK — provided crucial reassurance. Josephine reflected that consistent pathways, better communication, age-appropriate guidance, and support for key supporters would have significantly improved recovery.
2.2 Challenges and inequalities in cardiac arrest recovery
Despite improvements in life-saving interventions such as bystander CPR, post-cardiac arrest recovery remains inconsistent. Survivors and their key supporters, including family members, partners, friends, or anyone who witnesses or responds to the event, face a wide range of long-term and interrelated challenges.
Clinical challenges
- Ongoing cardiac issues, fatigue, reduced stamina, and mobility problems are common following cardiac arrest.
- Physical impacts are often long-term and poorly supported beyond hospital discharge.
- Access to specialist follow-up care and rehabilitation varies significantly by location and service availability.
Cognitive challenges
- Many survivors experience cognitive impairment, including memory loss, reduced concentration, slower information processing, and difficulties with planning and decision-making.
- These impairments can significantly affect independence, confidence, and the ability to return to work or education.
- Access to cognitive assessment and rehabilitation remains inconsistent and is often limited.
Psychological challenges
- Anxiety, depression, and post-traumatic stress disorder (PTSD) affect an estimated 15–30% of survivors.
- Psychological distress may be exacerbated by the traumatic nature of the cardiac arrest and uncertainty around recovery.
- Temporary loss of a driving licence, which for many becomes permanent, can further impact independence and emotional wellbeing.
- Key supporters may also experience anxiety, distress, and fear of recurrence, with limited access to tailored psychological support.
Social challenges
- Returning to work, driving, and maintaining relationships can be difficult for many survivors.
- Around 40% report ongoing physical limitations that affect daily life.
- Cognitive and psychological challenges can further hinder social reintegration and participation.
- Key supporters often face disruptions to employment, caring responsibilities, and family dynamics.
Economic challenges
- Survivors may experience reduced earning capacity, prolonged time off work, or early retirement.
- Families may face additional costs related to care, travel, or rehabilitation.
- Financial pressures are often more severe in already deprived households, reinforcing existing inequalities.
Inequalities across the cardiac arrest care pathway
- Inequalities persist across the entire cardiac arrest care pathway, from emergency response to post-discharge recovery and rehabilitation.
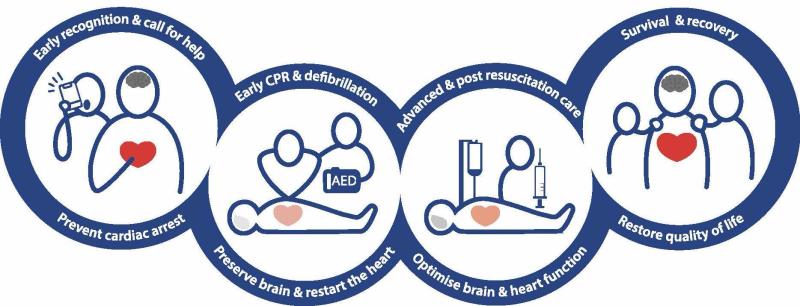
- Emergency response refers to the immediate recognition of cardiac arrest, calling emergency services, delivery of bystander CPR, and access to early defibrillation.
- Evidence from Europe shows ethnic and socioeconomic disparities in resuscitation outcomes, with minority ethnic groups and deprived communities experiencing lower survival rates due to delayed bystander intervention and reduced access to AEDs.10,11
- Available data shows that South Asian individuals are underserved by cardiac rehabilitation services, with lower uptake and completion rates compared to White British individuals.12 RCUK’s Every Second Counts report highlights the need for a CPR-trained society to help address these inequalities.13
2.3 Gaps in current care and support across the UK
While some regions offer specialist follow-up clinics and coordinated rehabilitation pathways, which have been shown to improve both physical and mental health outcomes, many survivors receive little or no structured support once discharged from hospital.
Inconsistent follow-up and rehabilitation
- Access to post-cardiac arrest rehabilitation varies significantly across the UK, resulting in marked regional disparities in care.
- Inequalities persist in access to rehabilitation, with evidence highlighting barriers such as poor communication between services and a lack of available resources.14
- Many survivors do not receive routine follow-up, multidisciplinary assessment, or timely referral to appropriate rehabilitation services.
System and clinician barriers
- Funding shortages limit the availability and sustainability of specialist clinics, rehabilitation programmes, and long-term support services.
- Clinician barriers, including limited capacity and infrastructure, hinder consistent delivery of post-cardiac arrest care.
- In particular, a lack of transport infrastructure to cardiac arrest centres presents a significant barrier for survivors requiring specialist follow-up15,16
Fragmented pathways and data gaps
- Poor coordination between acute care, community services, and primary care contributes to fragmented recovery pathways and inconsistent patient experiences.
- The absence of comprehensive UK-wide data on post-cardiac arrest outcomes and service provision limits the ability to identify gaps, evaluate impact, and drive systematic improvement.
Consequences of unmet need
- Gaps in post-cardiac arrest care reduce quality of life and increase the risk of long-term disability for survivors.17
- Inadequate rehabilitation and follow-up contribute to avoidable hospital readmissions and increased demand on health and social care services.18
- Significant economic costs that could be avoided through well-resourced, equitable and patient centred services.
10 L. Horriar, N. Rott, and B. W. Böttiger, “Improving Survival after Cardiac Arrest in Europe: The Synergetic Effect of Rescue Chain Strategies,” Resuscitation Plus 17 (2023): 100533, https://doi.org/10.1016/j.resplu.2023.100533.
11 I. Uny, K. Angus, and F. Dobbie, “Barriers and Facilitators to Delivering Bystander Cardiopulmonary Resuscitation in Deprived Communities: A Systematic Review,” Perspectives in Public Health 143, no. 1 (2022): 43–53, https://doi.org/10.1177/17579139211055497.
12 J. McAllister, M. Harrison, C. A. Lawson, and S. J. Singh, “Ethnic Health Inequalities in Cardiac Rehabilitation: Driving High-Quality Data,” British Journal of Cardiac Nursing 19, no. 7 (2024), https://doi.org/10.12968/bjca.2024.0095.
13 Resuscitation Council UK, Every second counts: Tackling inequalities in resuscitation, 2024, https://www.resus.org.uk/every-second-counts.
14 J. Eddison, O. Millerchip, A. Rosenberg, A. Lewinsohn, and J. Raitt, “Clinicians’ Experience of Barriers and Facilitators to Care Delivery of an Extracorporeal Cardiopulmonary Resuscitation Service for Out-of-Hospital Cardiac Arrest: A Qualitative Survey,” Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine 32 (2024): 86, https://doi.org/10.1186/s13049-024-01261-7.
15 J. Eddison et al, “Clinicians’ Experience of Barriers and Facilitators to Care Delivery”, 2024.
16 S. Katzenschlager, A. Elshaer, B. Metelmann, C. Metelmann, K. Thilakasiri, V. Karageorgos, T. Barry, K. Alm-Kruse, H. Karim, H. Maurer, J. Kramer-Johansen, and S. Orlob, “Top 5 Barriers in Cardiac Arrest Research as Perceived by International Early Career Researchers — A Consensus Study,” Resuscitation Plus 18 (2024): 100608, https://doi.org/10.1016/j.resplu.2024.100608.
17 G. M. Pound, C. Grimwood, A. Rix, K. Wickham, D. Jones, G. M. Eastwood, and C. L. Hodgson, “Long‑term Functional Outcomes and Health‑Related Quality of Life Following In‑Hospital Cardiac Arrest (IHCA): A Systematic Review,” Resuscitation 214 (2025): 110673.
18 K. N. Sawyer et al., “Sudden Cardiac Arrest Survivorship: A Scientific Statement from the American Heart Association,” 2020.